| ** | Latin American Journal of Clinical Sciences and Medical Technology is an open access magazine. To read all published articles and materials you just need to register Registration is free of charge. Register now If you already have registered please Log In | ** |




 0000-0002-5642-8255)a; Antonio Vicente Yam-Sosa (0000-0002-7499-1009)b; Mario Alberto Ramírez-Camacho (0000-0003-4152-3118)c; Miguel Güémez-Pineda (0009-0005-7955-2581)d; Gloria Uicab-Pool (0000-0001-7747-4245)b; Margarita Zarco-Salgado (0009-0007-9967-0846)e; Ligia Vera-Gamboa (0000-0001-6300-3549)f.
0000-0002-5642-8255)a; Antonio Vicente Yam-Sosa (0000-0002-7499-1009)b; Mario Alberto Ramírez-Camacho (0000-0003-4152-3118)c; Miguel Güémez-Pineda (0009-0005-7955-2581)d; Gloria Uicab-Pool (0000-0001-7747-4245)b; Margarita Zarco-Salgado (0009-0007-9967-0846)e; Ligia Vera-Gamboa (0000-0001-6300-3549)f.aLaboratorio de Bioquímica y Genética Molecular, Facultad de Química, Universidad Autónoma de Yucatán, Mérida, Yucatán, México; bFacultad de Enfermería, Universidad Autónoma de Yucatán, Mérida, Yucatán, México; cCentro de Información de Medicamentos y Farmacia Clínica, Facultad de Química, Universidad Autónoma de Yucatán, Mérida, Yucatán, México; dCentro de Investigaciones Regionales Dr. Hideyo Noguchi, Unidad Ciencias Sociales, Universidad Autónoma de Yucatán, Mérida, Yucatán, México; eUnidad de Proyectos Sociales, Universidad Autónoma de Yucatán, Mérida, Yucatán, México; fCentro de Investigaciones Regionales Dr. Hideyo Noguchi, Unidad Biomédica, Universidad Autónoma de Yucatán, Mérida, Yucatán, México.
Corresponding Author: , . Telephone number: ; e-mail: antonio.yam@correo.uady.mx

Lat Am J Clin Sci Med Technol. 2026 Apr;8:52-63.
Received: February 5th, 2026.
Accepted: April 21st, 2026.
Published: April 30th, 2026.
Views: 866
Downloads: 7

Introduction. Type 2 diabetes (T2D) is a multi-causal disease that requires approaches from various dimensions: biological, psychological, social, and cultural. Health is not only a bionatural process, but a complex social issue that needs to be studied, especially in disadvantaged populations such as those of Mayan descent from Yucatán, Mexico. Objective. To systematize the experiences in approaching the care to Mayan people with T2D in Yucatán from the perception of the opportunities and barriers faced by multidisciplinary teams that have worked in this population. Materials and Methods. The systematization of experiences was used as a methodology, through an orderly reconstruction process, to identify opportunities and barriers in the care of T2D. Critical interpretation was used with the intention of rescuing the most relevant learning. The techniques used for data analysis were the discussion group and content analysis. Results. The lessons learned about opportunities stand out: a transdisciplinary, multidisciplinary, and interinstitutional approach to diabetes, as well as comprehensive care. Among the barriers, a lack of communication in the Mayan language, a lack of sociocultural focus in research, and a lack of attention in the context of a pandemic (emergencies) were identified. Conclusions. The opportunities and barriers in addressing the care of Mayan people with T2D in Yucatán were framed in sociopolitical, educational, and sociocultural aspects.
Introducción. La diabetes tipo 2 (DT2) es una enfermedad multicausal que requiere abordajes desde varias dimensiones: biológica, psicológica, social y cultural. La salud no es sólo un proceso bionatural, sino un tema social complejo que necesita ser estudiado, especialmente en poblaciones desfavorecidas como las de ascendencia maya de Yucatán, México. Objetivo. Sistematizar las experiencias en el abordaje de la atención de los mayas con DT2 en Yucatán, desde la percepción de las oportunidades y barreras de los equipos multidisciplinarios que han trabajado en esta población. Material y métodos. Se utilizó como metodología la sistematización de experiencias mediante un proceso de reconstrucción ordenada, que permitió identificar oportunidades y barreras en la atención de la DT2. Se utilizó la interpretación crítica con la intención de rescatar los aprendizajes más relevantes. Las técnicas utilizadas para el análisis de datos fueron el grupo de discusión y el análisis de contenido. Resultados. Se destacan los aprendizajes sobre oportunidades: el abordaje de la diabetes con un enfoque transdisciplinario, multidisciplinario e interinstitucional, así como la atención integral. Entre las barreras se identificaron la falta de comunicación en lengua maya, la falta de enfoque sociocultural en la investigación y la falta de atención en el contexto de una pandemia (emergencias). Conclusiones. Las oportunidades y barreras para abordar la atención de las personas mayas con DT2 en Yucatán se enmarcaron en aspectos sociopolíticos, educativos y socioculturales.
In Mexico, type 2 diabetes (T2D) is associated with a multiplicity of conditions, such as the aging process, genetics, the environment, and culture, which interact in a complex way, resulting in a vertiginous increase in the disease.1
Although the conditions that underlie diabetes are similar throughout the country, there are differences among certain population groups, such as the diverse indigenous groups that inhabit Mexico, since they live in particular social environments.2
A constant that can be seen in the indigenous communities is the shared disadvantage in terms of health and social situation. Reframing diabetes within a paradigm of social and cultural determinants of health reveals diabetes as a product of unjust circumstances and environments, rather than a disease based solely on pathology and individual responsibility.
In addition, significant barriers to care for indigenous peoples, such as fragmented healthcare, poor management of chronic illnesses, and limited or no health surveillance3 complicate the T2D management in disadvantaged populations.
In Yucatán, Mexico, Universidad Autónoma de Yucatán (UADY) is the university with the largest presence in the region. The Social Projects in Learning Communities (SPLC), coordinated by UADY over the last eight years, constitute the empirical basis of the present study; specifically, they serve as the 'social laboratory' from which the systematized evidence analyzed here emerged. Rather than functioning as a conventional community service or administrative strategy, these projects serve as a longitudinal, immersive observational framework for healthcare practices directed at Mayan populations with T2D. This approach deliberately integrates academic knowledge with community-based expertise through a continuous process of critical feedback and systematization of experiences. SPLCs are a strategy put in place to achieve the commitment and social responsibility of graduates and future professionals by addressing the problems and pressing needs of communities, as is the case with T2D.4
According to the 2020 National Population Census, Yucatán accounts for 23.8% of the national Mayan-speaking population, with approximately 537,516 speakers. This linguistic and ethnic distinctiveness represents a structural barrier to equitable access to healthcare services, as a significant proportion of people with T2D attending health centers in rural communities primarily communicate in the Mayan language, thereby limiting the quality of clinical care.5,6
The SPLC has implemented care programs for people living with T2D in the Mayan population of Yucatán in municipalities located in the south of the state, where 83.2% of the population is in a situation of poverty, 31.1% have an index of deficiencies due to access to food, and 91.82% consider themselves indigenous.5,6
This growing scientific and academic interest can be attributed to the convergence of at least three interrelated processes:
- The accelerated nutritional transition observed in numerous indigenous communities over the last two decades, characterized by the progressive replacement of traditional dietary patterns with ultra-processed food and the adoption of markedly sedentary lifestyles7;
- The structural limitations of the hegemonic biomedical model, whose predominantly individual and clinical approach has proven insufficient to address the multi-causal and socially determined nature of T2D in culturally and linguistically diverse contexts5; and
- The documented and disproportionate increase in T2D prevalence in indigenous populations, particularly in children and youth, which in various contexts exceeds the national population average by 1.5 to 2 times.
However, in these investigations (both biomedical and social), a unidisciplinary biomedical approach has predominated. Therefore, there have been few multidisciplinary approaches and even fewer interdisciplinary approaches.
In this context, the purpose of this work was to identify the barriers and opportunities in the approach to people living with T2D in Yucatecan Mayan communities in Mexico, their families, and other actors involved through the systematization of the approaches proposed in a set of investigations coordinated by AUDY academics in the last eight years.4
The findings of this study may be useful for future research on T2D in rural contexts where the described social determinants may be similar.
The systematization of experience was adopted as the guiding epistemological and methodological framework for this study. This approach —deeply rooted in the Latin American tradition of popular education and participatory research— involves the critical, reflexive, and orderly reconstruction of an intervention process. Its objective is to identify lessons learned and generate transferable knowledge derived directly from practice.9
Unlike a simple description or a traditional literature review, the systematization of experience seeks to understand the 'why' and 'how' of what occurred. This allows participants to become rather than merely subjects of study.10
Content analysis was subsequently employed as the analytical technique for processing the discursive material generated by professionals during the systematization sessions, ensuring coherence with the overarching framework.
The study was carried out from March to November 2021. This methodology focused on understanding the methodological processes developed in various community projects in the approach to care for Mayan people with T2D in Yucatán.
The systematization supposes different moments of analysis, although not always in a linear way. Thus, the systematization experience presented was considered to consist of four stages.11
Content analysis was conducted following a thematic-categorical approach.12
The process was developed in three sequential phases to ensure data traceability:
- Open coding, where transcriptions from the three seminar sessions were read line-by-line to assign initial codes to significant discursive units related to barriers or opportunities;
- Axial coding, where codes with conceptual affinity were grouped into preliminary categories, and
- Selective coding, where four general subcategories were constructed through research team consensus: sociocultural, economic, sociopolitical, and educational.13
Categorical saturation served as the criterion to validate the comprehensiveness of the subcategory system.
To ensure reliability, two researchers independently coded 20% of the material; the inter-coder agreement was calculated using the Kappa coefficient (κ = 0.82), indicating substantial reliability and high consistency in the coding process.14
This systematic approach supports the rigor and trustworthiness of the transition from a raw professional discourse to the final analytical categories.
First stage
The object of knowledge was identified and built based on the barriers and opportunities present in the care given to people with T2D.
The barriers and opportunities were identified by professionals from different disciplines involved in SPLCs as they operationalized their projects within their respective working communities. To do so, it was necessary to focus on aspects of the dialogic process that were generated.
Through a virtual seminar titled "Advances in the Approach to Caring for People with T2D in the Mayan Area of the Yucatán Peninsula", which consisted of three sessions (each lasting two hours), each professional presented the main results obtained during the operationalization of their projects.
Additionally, they answered two questions that were the guide for obtaining data for the study: What are the barriers and opportunities that you identify from your experience?
Second Stage
The actors were identified, that is, the professionals who implemented the programs and projects for the care given to Mayan people with T2D.
The participant population comprised 11 projects: six in the eastern region and five in Southern Yucatán, Mexico.
These projects were implemented by professionals from various disciplines in the areas of health and social sciences.
The projects include the following disciplines: Biology-Pharmaceutical, Nursing, Medicine, Nutrition, Chemical Engineering, and, in the second, Medical Anthropology and Social Work.
Third Stage
It was necessary to clarify the context in which the projects were developed and the interest in systematizing the insights and experiences gained from the AUDY SPLC. These were clarified to build on insights and experiences, with the vision of proposing a model with a comprehensive focus on providing care for people with diabetes in the Mayan area of the Yucatán Peninsula.
In addition, systematization, as a process, will provide feedback on what has been done and improve approaches.11
Fourth Stage
The techniques for analyzing the systematization process were selected, taking into account the use of content analysis.12,13
The units of analysis comprised words related to opportunities and barriers, according to the conceptualization the investigating authors identified during the operationalization of their projects.
The context unit was based on the social dimensions to which each of the opportunities and barriers identified in each project corresponded.
Likewise, subcategories identified in each professional group were built and met the relevant requirements, that is, that the projects were appropriate for the purposes of the study.
The subcategories identified were sociocultural, economic, sociopolitical, and educational. These were comprehensive, as they were recognized in each of the professions identified in the projects reviewed. We grouped them by the nature of their associated projects to standardize them across professional disciplines for analysis.
To quantify the analysis subcategories (categorical weights), the number and percentage of records that appeared in each subcategory were counted to detect possible barriers and opportunities (Table 1). This involved analyzing interdisciplinary interactions.15
| Table 1. Categorical weight of barriers and opportunities by subcategory and frequency of appearance in the 11 analyzed projects | |||||
|---|---|---|---|---|---|
| Subcategory | Category | Specific barrier or opportunity | Frequency (n) | Projects (%) | Disciplines that identified it |
| Sociocultural | Barrier | Communication (Mayan language) | 11 | 100.0 | All disciplines |
| Sociopolitical | Barrier | Lack of sociocultural focus in research | 9 | 81.8 | Nursing, Anthropology, Social Work, Medicine |
| Professional Educational | Barrier | Lack of comprehensive medical training; lack of disciplinary interest in research | 2 | 13.3 | Medicine and Nutrition |
| Sociopolitical | Opportunity | Multidisciplinary and inter-institutional approach | 10 | 90.9 | All disciplines |
| Educational | Opportunity | Inclusive language training | 8 | 72.7 | Nursing, Medicine, Pharmaceutical Chemistry |
| Sociocultural | Opportunity | Self-management with gender and intercultural focus; traditional medicine; sociocultural training | 5 | 27.8 | Nursing, Nutrition, and Pharmaceutical Chemistry |
| Formative Educational | Opportunity | Values education; student training; telemedicine | 4 | 22.2 | Nursing and Pharmaceutical Chemistry |
| Source: Own elaboration based on study data. | |||||
To facilitate their reading and interpretation, they were placed in a matrix, where the rows represented the barriers and opportunities, and the columns represented the disciplines.
To depict the interdisciplinary interactions between barriers, opportunities, and professional disciplines, Sankey diagrams were generated using the open-source framework RAWGraphs 2.0. This tool was selected for its ability to visualize the 'flow' and distribution of categorical data across multiple dimensions.
Unlike static matrices, the Sankey diagram allows for an explicit mapping of how specific barriers and opportunities are distributed across the participating disciplines, with the width of the links (edges) proportional to the frequency of identification.
The Sankey representation is methodologically aligned with the systematization of experience, as it highlights the weight of shared knowledge versus discipline-specific insights, facilitating the identification of cross-cutting nodes—such as linguistic barriers—that were recognized by the entire multidisciplinary team.
Ethical Considerations
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki (revised in 2013) and the General Health Law on Research in Mexico.16,17 The study protocol was approved by the Bioethics Committee of the Project Registration System (SISTPROY) from Universidad Autónoma de Yucatán (Registration No. CIRS 2022-0006).
All professionals who participated in the seminar sessions were informed of the study's purpose and provided written informed consent for their testimonies to be recorded, systematized, analyzed, and published.
No personally identifiable information was collected; testimonies were anonymized during analysis to ensure confidentiality by using the discipline’s name as the only identifier (e.g., Nursing, Anthropology, Social Work, Medicine, Nutrition, Pharmaceutical Chemistry) (Table 2).
| Table 2. Professional arguments organized by categories and subcategories | |||
|---|---|---|---|
| Subcategory | Category | Specific barrier or opportunity | Argument (direct quote) |
| Sociocultural | Barrier | Communication (Mayan language) | “One of the first things we noticed was that people with diabetes did not understand the instructions we gave them... many of them think in Maya, and since we don’t know Maya, we couldn’t communicate effectively.” (Nursing) |
| “The barrier is not only linguistic but also conceptual. Diabetes is not explained or understood the same way in Maya as it is from a biomedical language.” (Anthropology) | |||
| Sociopolitical | Barrier | Lack of sociocultural focus in research | “We continue to design research from an external logic, without starting from how communities live and signify diabetes.” (Social Work) |
| “Medical ethnocentrism is still very much present; even in indigenous contexts, the biomedical model ends up imposing itself.” (Medicine) | |||
| Professional Educational | Barrier | Lack of comprehensive medical training | “Our training was very clinical, very technical, but it did not prepare us to work with diabetes as a social and community problem.” (Medicine) |
| Sociopolitical | Opportunity | Multidisciplinary approach | “When we work together across disciplines... we stop seeing diabetes as an isolated problem and start addressing it comprehensively.” (Nursing) |
| Educational | Opportunity | Inclusive language training | “Changing the way we talk to patients completely transformed the relationship with them; there was more trust and greater adherence.” (Medicine) |
| Sociocultural | Opportunity | Intercultural self-management | “When we incorporated traditional medicine and local food, people became more involved in their own care.” (Nutrition) |
| Formative Educational | Opportunity | Student training | “Training students with a sociocultural focus changed the way they approach and address community work from the very beginning.” (Nursing) |
| Source: Own elaboration based on study data. | |||
Given that this study involved the retrospective analysis of academic practice experiences—rather than direct experimentation with human subjects or sensitive clinical data—it was classified as 'minimum risk' research according to current Mexican regulations.
Based on the study's findings, the characteristics of the systematized projects, as well as opportunities and barriers related to experience with the approach to providing care for people with T2D in the Mayan area of Yucatán, are presented.
Characteristics of the Participatig Projects
These were university social projects that were developed in localities in the eastern part of the state of Yucatán, Mexico: Tixcacaltuyub, Yaxcabá, and Tizimín. These are localities of Mayan origin where social determinants shape the living conditions of the population, including people with T2D and their families.
Eleven projects carried out between 2014 and 2021 were analyzed. All of them address the T2D phenomenon, and their results focus on the range of the clinical variable, glycosylated hemoglobin (<7%), which was used as a result indicator. The primary and secondary variables included family support, healthy eating, medication use, and workshops training participants in disease management skills.
After a detailed analysis of the projects' results, it was observed that one project included a comparison and an experimental group, while three projects used a quasi-experimental methodology with pre- and post-intervention measurements.
The objective of one of these three projects was to develop a prototype tool for patients with T2D that integrates metabolic control and genetic information into the VIADAT platform to identify possible metabolic responses.
The second project addressed the prevalence of diabetes in the community, and the third described the clinical and anthropometric indicators among users of the diabetes control program at the primary care center in the study community.
Six of the projects present their results with a qualitative methodology, where they analyze multiple phenomena such as emotions based on the experience of living with the disease, the experience of living with some complication caused by diabetes, the perception towards the diet used to live with the disease, and the adaptation to the various factors that hinder the proper management of the disease.
The interventions described in the projects were implemented over 1 to 3 years to achieve their objectives.
A disciplinary approach was observed in Nursing and Social Work, whilst they also engaged in collaborative work with Medicine and Psychology. On the other hand, collaborative work between Medicine, Nutrition, Chemical-Pharmaceutical, Psychology, and Engineering was also observed.
It is possible that the interaction occurred due to the very nature of the project; that is, the proposed objectives required the specific skills of the professionals that make up the team. It may also have depended on the external origin of the resource that financed the project and required multidisciplinary work.
In projects with a single-discipline approach, funding was internal, and there was no requirement for inter-disciplinary collaboration.
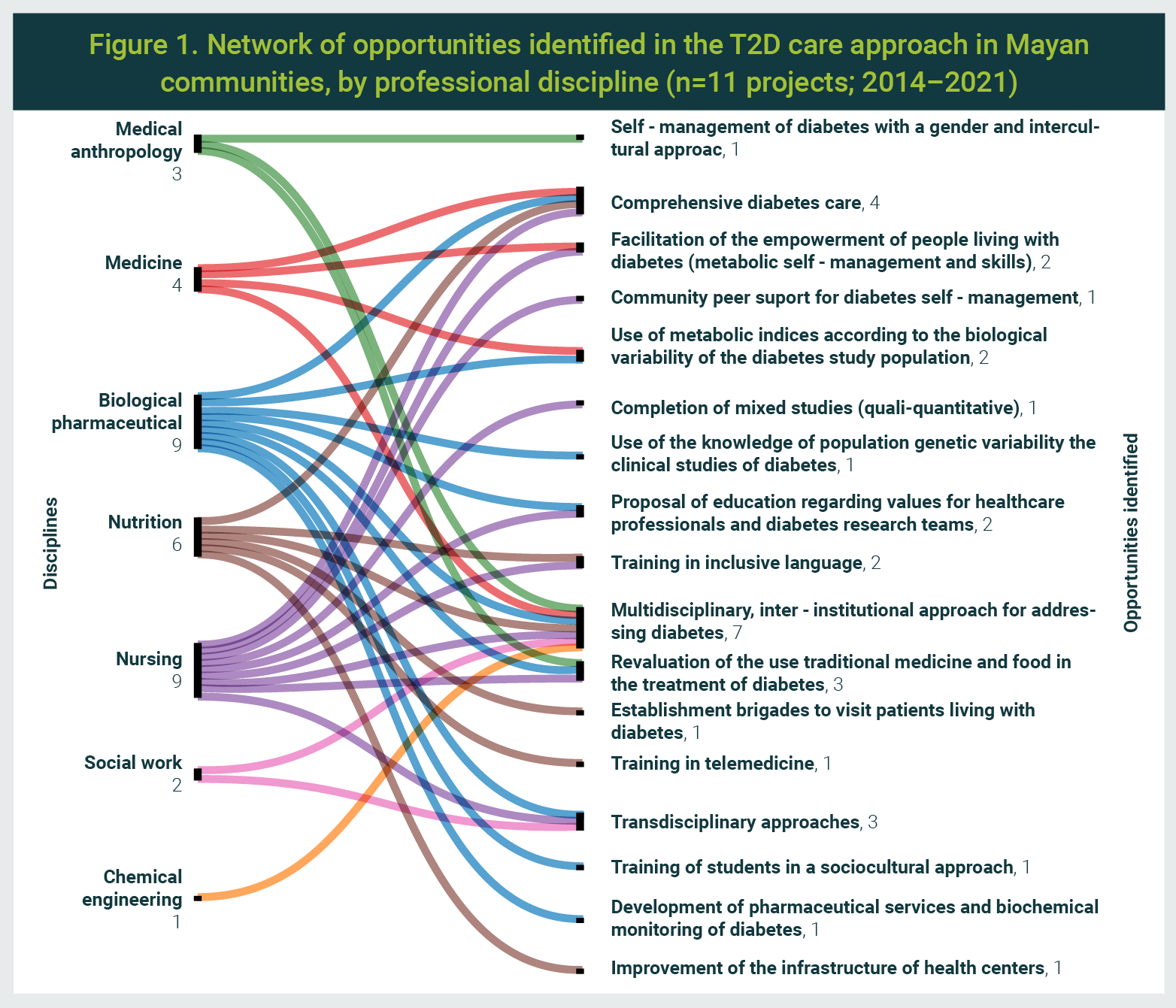
Opportunities
Social dimensions corresponding to four subcategories were identified, with categorical weights: education, sociopolitics, sociocultural, and economics.
Education
Arguments that refer to or allude to professionals' conceptualization of diabetes education: a comprehensive education that promotes empowerment for self-management of the disease, with inclusive language, a gender perspective, and an intercultural approach.
In addition, the educational process must include clinical studies using metabolic rate, accounting for biological and genetic variability, and mixed studies, that is, studies with both qualitative and quantitative paradigms. At the same time, health professionals who provide diabetes education must be trained in the values, skills, and attitudes relevant to the sociocultural contexts of people living with diabetes.
Sociopolitics
Arguments that allude to a series of transformations and changes in which people with diabetes should be guided, that is, with comprehensive care, a multidisciplinary and inter-institutional approach, as well as the reevaluation of the use of traditional medicine and food in the treatment of diabetes.
It also includes establishing brigades for home visits to people with diabetes, as well as the use and promotion of telemedicine for training among health professionals and with people with diabetes in the community.
Sociocultural
Arguments to which reference is made or that allude to how to meet the needs of the population transdisciplinarily, as well as establishing effective transdisciplinary communication between the actors.
In addition, professionals point out that students who participate in community projects must have training with a sociocultural focus.
Economics
Statements on emerging or alternative practices, such as the development of pharmaceutical services and biochemical monitoring of diabetes, as well as the improvement of the infrastructure of the health centers in the communities where the projects are implemented, and related to better service.
Figure 1 presents the opportunities identified by each discipline and among them.
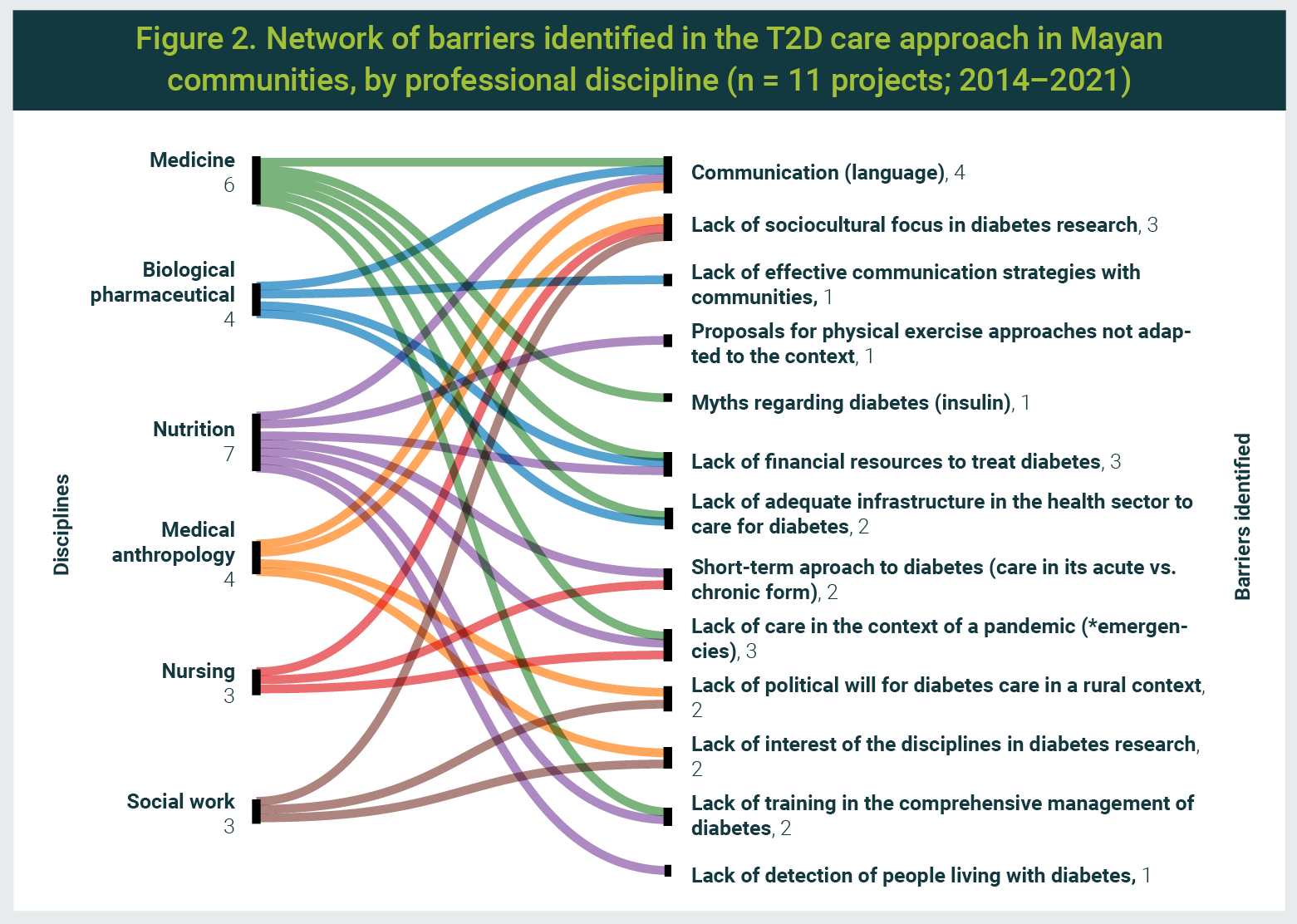
Barriers
Social dimensions corresponding to four subcategories were identified, based on categorical weight: sociocultural, economic, sociopolitical, and educational.
Sociocultural
Arguments that allude to a series of situations that interfere with communication (language), such as:
- the lack of a sociocultural approach in diabetes research (medical ethnocentrism),
- the dominant predominance of the biomedical paradigm, and
- the absence of effective communication strategies between health professionals and people from the communities.
Further examples include practices taught outside the community context, such as approaches to physical exercise, and the incorporation of myths into diabetes care (e.g., insulin use) by those living with the disease.
Economics
Arguments that refer to professionals' perceptions of the approach to providing care for people with T2D, such as the lack of economic resources and the absence of personnel (nutritionists and social workers, among others) to provide services in health centers.
Sociopolitics
Professionals' perceptions of the current situation in the approach to diabetes. This includes a lack of care during a pandemic (an emergency), inadequate health sector infrastructure to address T2D, and a lack of political will among health authorities to provide care to individuals with T2D in rural contexts. Additionally, it includes the existence of a short-term approach to diabetes (care in its acute vs. chronic form).
Education
Statements by professionals about the consequences regarding the care of the individual with T2D, such as the lack of interest of the disciplines in research and medical training for comprehensive management, as well as the lack of detection of people with T2D.
Figure 2 presents the barriers identified by each discipline and among them.
One of the study's findings highlights the multidisciplinary approach as an opportunity; that is, the professionals report that T2D is a complex and challenging disease for the individual who suffers from it because it requires daily self-control decisions. Consequently, education and support for self-management of the disease encompass a comprehensive combination of clinical, educational, psychosocial, and behavioral aspects, forming the basis for helping and collaborating with people. This is possible when there is a team of professionals trained in education and disease management.18
Thus, the multifactorial nature of diabetes, its care, and clinical treatment account for only 10-20% of the modifiable contributors to disease outcomes, with the remaining 80-90% related to social determinants of health, including health-related behaviors, socioeconomic factors, environmental factors, discrimination, and racism.19
One criterion to consider when creating multidisciplinary diabetes care teams is the representativeness of the communities they serve.
If the population where the programs are implemented is identified as Mayan-speaking, the health team professionals must identify themselves as from the same region where this group lives. This situation will contribute to an acceptance and understanding of the situation of people with diabetes.16
Another opportunity reported in the study, Comprehensive Care for Diabetes, is the importance of institutionality, as it is part of comprehensive care. For this to be achieved, the approach must be based on the needs of each person living with the disease. Therefore, efforts to improve population health will require a combination of approaches at the policy, systems, and patient levels.19,20
Faced with the challenge of combining approaches, the importance of patient-centered care is highlighted and defined as care that considers the person's individual comorbidities and prognoses, as well as being respectful and receptive, and ensuring respect for the preferences, needs, and values of the person; and ensuring that people's values guide all clinical decisions.19
On the other hand, the Social Determinants of Health (SDOH) are outside individuals' direct control and can pose lifelong risks, contributing to medical and psychosocial outcomes that must be addressed to improve overall health.21
Furthermore, biological and genetic variability should be included in T2D care programs. This means studies using both qualitative and quantitative paradigms, in which the health professionals who participate in the diabetes education process must be trained in the values, skills, and attitudes present in the sociocultural contexts of people with diabetes in Mayan communities.
In addition, traditional medicine and local food should be revalued in the treatment of diabetes; brigades for home visits to people with diabetes should be established; and the use of telemedicine for training among health professionals and people with diabetes in the community should be promoted. This is especially the case in emergency contexts, such as the recent COVID-19 pandemic or other natural disasters that these rural communities may suffer.
Another outstanding opportunity is the importance of the use of inclusive language with a gender perspective and an intercultural approach by health professionals who care for non-Mayan-speaking people, since they must develop or offer educational programs and materials with the mission of preventing diabetes and being aware of the differences in the teaching-learning processes involved in the transmission of knowledge. This is to reduce language barriers by improving cultural competence, addressing health literacy, and ensuring communication with language assistance.
Moreover, an opportunity to innovate arises when considering a website that offers various resources and materials to improve the quality of care in the provision of services to Mayan-speaking people. An example of this is the Culturally and Linguistically Appropriate Services (CLAS), which offer a variety of resources and materials to improve the quality of care for non-English speakers.22
Finally, the transdisciplinary approach was identified as an opportunity and is related to the inter-institutional opportunity to include the SDOH, as indicated by the American Diabetes Association (ADA) in its 2022 edition regarding the diabetes care approach. It is crucial that health professionals not only focus on the power their interventions have to improve equity but also on addressing non-medical social needs within the communities they serve.20
Barriers
The use of the systematization methodology led to the identification of factors that hinder the level of care afforded to people living with diabetes.
The experiences were critically interpreted, based on their arrangement, in addition to allowing the discovery, identification, and explanation of the logic of the process experienced, the factors that have intervened in said processes, how they have been related to each other, and why they have been done in that way.
The main barrier identified in this systematic analysis was related to the language used between healthcare personnel and people with diabetes in the Mayan communities of Yucatán.
It is known that, at the historical, linguistic, and ethnographic levels, there are linguistic discrepancies in the context of medical practice.22
Medical care is faced, as is the case of the time in Yucatán, Mexico, with the fact that the population to which it serves contains differentiated ethnic and linguistic characteristics.23
Although in most communities with a medical unit, bilingual personnel from the area are hired as auxiliaries to serve as interpreters or cultural interlocutors, there is always a risk of bias when conveying the message between the doctor and the patient.23
Therefore, it is necessary to develop measures and strategies to address language barriers in the provision of care to people living with diabetes in the Mayan communities of Mexico.22,23
Another barrier identified was the lack of political will among the authorities in the Yucatán health sector to support care for T2D in a rural context. This barrier is evident in a health system that is often fragmented, lacks clinical information capabilities, has duplicated services, and has a deficient design for the coordinated care of people with any chronic condition. To address this situation, the Chronic Care Model (CCM) is an effective framework for improving the quality of care for people with diabetes.24
Besides identifying barriers in the analyzed projects, more importantly, opportunities were observed to present an indicator of social relevance, which is the recognition and revaluation of the local knowledge of the participating population: their practices, experiences, and values, which are, in themselves, a fundamental part of the authors' proposals.
Although professionals encounter barriers in implementation, social projects have contributed to the empowerment of the communities where they have been implemented.
The participatory methodologies adopted for social intervention enabled the inhabitants of the communities to, in collaboration with university professionals, decide on work priorities, the issues in their lives that needed to be addressed, and action strategies, as well as the organizational process for executing tasks and evaluating them. That is, the community's perception of achievement.
The systematization of eight years of experience in addressing T2D in Mayan communities in Yucatán revealed that both the barriers and opportunities identified by multidisciplinary teams are organized around four interrelated social dimensions: sociocultural, economic, sociopolitical, and educational.
This finding directly addresses the study's objective and confirms that T2D in indigenous contexts cannot be effectively managed solely through a unidisciplinary biomedical perspective.
The interdisciplinary convergence of the identified barriers and opportunities—particularly the linguistic barrier and the opportunity for multidisciplinary care, both recognized by all participating professional fields—demonstrates that a multidisciplinary approach not only enriches the diagnostic understanding of the problem but also constitutes a methodological and ethical necessity for any intervention seeking cultural and epidemiological relevance within Mayan communities.
To Fajardo-Niquete and González-Basulto Freddy for their contribution to critical review. To Joseph Hill for the English grammar revision.
The authors declare that there is no conflict of interest.
| 1. | Romero-Martínez M, Shamah-Levy T, Vielma-Orozco E, Heredia-Hernández O, Mojica-Cuevas J, Cuevas-Nasu L, et al. Encuesta Nacional de Salud y Nutrición 2018-19: metodología y perspectivas. Salud Publica Mex. 2019;61(6):917-923. [Consultado el 22 de abril, 2026]. Disponible en URL: https://www.saludpublica.mx/index.php/spm/article/view/11095 |
| 2. | Buichia Sombra FG, Miranda Cota GA. Determinantes sociales de la salud y riesgo de diabetes tipo 2 en adultos de poblaciones originarias, aproximaciones desde la teoría social. J Acad. 2021;(4):227-51. [Consultado el 22 de abril, 2026]. Disponible en URL: https://journalacademy.net/index.php/revista/article/view/45 |
| 3. | Stephens C, Porter J, Nettleton C, Willis R. Disappearing, displaced, and undervalued: A call to action for indigenous health worldwide. Lancet. 2006;367(9527):2019-28. |
| 4. | Sáenz C, Zarco M. Extensión y responsabilidad social. Los proyectos sociales en comunidades de aprendizaje implementados en la Universidad Autónoma de Yucatán. México: Universidad Autónoma de Yucatán; 2015. p. 490. |
| 5. | Pelcastre-Villafuerte BE, Meneses-Navarro S, Sánchez-Domínguez M, Meléndez-Navarro D, Freyermuth-Enciso G. Condiciones de salud y uso de servicios en pueblos indígenas de México. Salud Publica Mex. 2020;62(6, Nov-Dic):810-819. [Consultado el 22 de abril, 2026]. Disponible en URL: https://www.saludpublica.mx/index.php/spm/article/view/11861 |
| 6. | Instituto Nacional de Estadística y Geografía (INEGI). Censo de Población y Vivienda 2020. México: INEGI; 2021. [Consultado el 22 de abril, 2026]. Disponible en URL: https://www.inegi.org.mx/programas/ccpv/2020/ |
| 7. | Barquera S, Hernández-Barrera L, Trejo-Valdivia B, Shamah T, Campos-Nonato I, Rivera-Dommarco J. Obesidad en México, prevalencia y tendencias en adultos. Ensanut 2018-19. Salud Publica Mex. 2020; 62(6): 682-692. [Consultado el 22 de abril, 2026]. Disponible en URL: https://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0036-36342020000600682 |
| 8. | Papadimos ER, Claussen C, Magliano DJ, Hotu C, Brown A, Pearson O, et al. Prevalence of youth type 2 diabetes in global Indigenous populations: A systematic review. Diabetologia. 2026;69(3):568-581. |
| 9. | Jara Holliday O. (s. f.). Orientaciones teórico-prácticas para la sistematización de experiencias. Biblioteca Electrónica sobre Sistematización de Experiencias, CEAAL. [Consultado el 22 de abril, 2026]. Disponible en URL: http://biblioteca.udgvirtual.udg.mx/jspui/bitstream/123456789/3845/1/Orientaciones_teorico-practicas_sistematizar_experiencias.pdf |
| 10. | Barnechea García MM, Morgan Tirado ML. La sistematización de experiencias: producción de conocimientos desde y para la práctica. Tendencias y Retos. 2010;15(1):97-107. [Consultado el 22 de abril, 2026]. Disponible en URL: https://revistas.lasalle.edu.co/index.php/te/article/view/4824 |
| 11. | Tapella E, Rodriguez-Bilella P. Sistematización de experiencias: una metodología para evaluar intervenciones de desarrollo. Rev Eval Programas Polit Publicas. 2014;(3):80-116. [Consultado el 22 de abril, 2026]. Disponible en URL: https://revistas.uned.es/index.php/REPPP/article/view/13361 |
| 12. | Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15(3):398-405. [Retrieved on April 23rd, 2026]. Available from URL: https://onlinelibrary.wiley.com/doi/epdf/10.1111/nhs.12048 |
| 13. | Creswell JW, Creswell JD. Research design: Qualitative, quantitative, and mixed methods approaches. Fifth ed. SAGE Publications; 2018. p. 304. |
| 14. | Andréu Abela J. Las técnicas de análisis de contenido: una revisión actualizada. España: Fundación Centro Estudios Andaluces, 2011. [Consultado el 22 de abril, 2026]. Disponible en URL: https://perio.unlp.edu.ar/tif/wp-content/uploads/2021/04/S200103-Las-tecnicas-de-Analisis-de-Contenido-Una-revision-actualizada.pdf |
| 15. | Luque Martín A, González Requena V. La salud está en tu mano: sistematización de experiencias sobre derecho a la salud en contextos educativos. España: Programa “La salud está en tu mano”, Farmamundi; 2018 [Consultado el 5 de mayo, 2026]. Disponible en URL: https://lasaludestaentumano.es/programa/ |
| 16. | World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. |
| 17. | Reglamento de la Ley General de Salud en Materia de Investigación para la Salud. (2 de abril, 2014). Diario Oficial de la Federación. [Consultado el 23 de abril, 2026] Disponible en URL: https://www.diputados.gob.mx/LeyesBiblio/regley/Reg_LGS_MIS.pdf |
| 18. | Powers MA, Bardsley JK, Cypress M, Funnell MM, Harms D, Hess-Fischl A, et al. Diabetes self-management education and support in adults with type 2 diabetes: A consensus report of the American Diabetes Association, the Association of Diabetes Care & Education Specialists, the Academy of Nutrition and Dietetics, the American Academy of Family Physicians, the American Academy of PAs, the American Association of Nurse Practitioners, and the American Pharmacists Association. Diabetes Care. 2020;43(7):1636-1649. |
| 19. | American Diabetes Association. 4. Comprehensive medical evaluation and assessment of comorbidities: Standards of medical care in diabetes—2021. Diabetes Care. 2021;44(Suppl 1):S40-S52. |
| 20. | American Diabetes Association Professional Practice Committee. 1. Improving care and promoting health in populations: Standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S8-S16. |
| 21. | Haire-Joshu D, Hill-Briggs F. The next generation of diabetes translation: A path to health equity. Annu Rev Public Health. 2019;40:391-410. |
| 22. | U.S. Department of Health & Human Services. Office of Minority Health. National Standards for Culturally and Linguistically Appropriate Services (CLAS) in Health and Health Care. Washington, DC: HHS, 2021. Available from URL: https://thinkculturalhealth.hhs.gov/clas |
| 23. | Dickinson JK, Guzman SJ, Maryniuk MD, O'Brian CA, Kadohiro JK, Jackson RA, et al. The use of language in diabetes care and education. Diabetes Care. 2017;40(12):1790-1799. |
| 24. | Jacobs EA, Lauderdale DS, Meltzer D, Shorey JM, Levinson W, Thisted RA. Impact of interpreter services on delivery of health care to limited-English-proficient patients. J Gen Intern Med. 2001;16(7):468-74. |
All Rights Reserved® 2019
Latin American Journal of Clinical Sciences and Medical Technology,Publicación contínua • Editor responsable: Gilberto Castañeda Hernández. • Reserva de Derechos al Uso Exclusivo: 04-2019-062013242000-203; ISSN: 2683-2291; ambos otorgados por el Instituto Nacional del Derecho de Autor. • Responsable de la última actualización de este número, Web Master Hunahpú Velázquez Martínez,
Calle Profesor Miguel Serrano #8, Col. Del Valle, Alcaldía Benito Juárez, CP 03100, Ciudad de México, México. Número telefónico: 55 5405 1396 • Fecha de última modificación, 28 de agosto de 2024.
All Rights Reserved® 2019
Publicación contínua • Editor responsable: Gilberto Castañeda Hernández. • Reserva de Derechos al Uso Exclusivo: 04-2019-062013242000-203; ISSN: 2683-2291; ambos otorgados por el Instituto Nacional del Derecho de Autor. • Responsable de la última actualización de este número, Web Master Hunahpú Velázquez Martínez,
Calle Profesor Miguel Serrano #8, Col. Del Valle, Alcaldía Benito Juárez, CP 03100, Ciudad de México, México. Número telefónico: 55 5405 1396 • Fecha de última modificación, 28 de agosto de 2024.